 |
 |
 |
Public Health,
Epidemiology, and Cervical Cancer Research in At-Risk
Communities
Rates of cancer are directly impacted by strong public
health policies that educate patients and provide access
to free screenings or tests. In the United States, the
Pap test helped reduce rates of cervical cancer by at
least 70% since the 1950s [1]. Cervical cancer was once
the leading cause of cancer-related death in American
women. It now has a five-year survival rate of
more than 65%, a landmark
achievement in public health.
The recognition of cancer as a public health issue,
particularly in underserved, low-income communities, was
an important moment in US medical history. This was
driven by epidemiological research analyzing disease
frequency in relation to various demographic and
socioeconomic factors including race, ethnicity, income,
geographic location, age, sex and more.
These studies had been used for decades to track
infectious disease, but their application to
noninfectious disease, like cancer, was relatively new
in the 1960s. When applied to cervical cancer, the
studies almost uniformly found that the highest rates of
cervical cancer were concentrated in poor and/or
minority communities with low rates of Pap testing
[2-6]. These early studies called for public health
efforts aimed at educating patients and physicians on
the benefits of Pap testing to diagnose cervical cancer
at earlier, nonterminal stages.
In the 1960s many American physicians were still
skeptical of the Pap test and did not always recommend
it for their patients. For instance, a 1960-62 survey of
2,000 women in San Diego found that 93% had never been
told to have a Pap test by a doctor [5]. This was
remarkable, as the Pap test had been used in the United
States for some time and was considered a standard
screening tool.
By the 1970s, Pap testing was more frequent for all
women in the US, leading to reduced cervical cancer
rates and deaths [7]. But epidemiological studies
surrounding these factors were lacking, as most
large-scale studies were focused on separating groups by
age and stage of cancer diagnosis [7] but not other
factors.
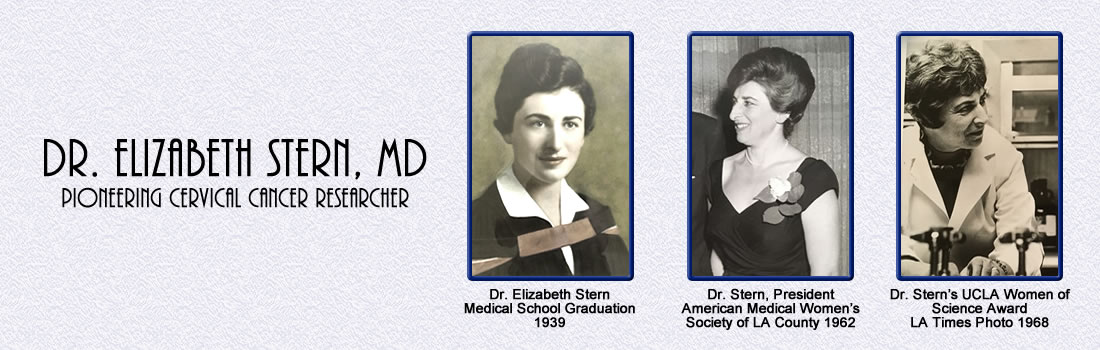
Dr. Stern’s research on cervical cancer in the 1970s
involved innovative epidemiological studies in
vulnerable communities. Her focus on effective,
community-based clinical outreach and empathy for
patients, unique at the time, provided strategies for
setting up successful cervical cancer screening clinics.
Identifying Communities with High Rates of Cervical
Cancer
Epidemiological studies in the 1960s generated new
public health policies, and as a result, cervical cancer
rates nationwide were decreasing. But were rates
decreasing among the most vulnerable communities? Few
studies focused solely on low-income and/or
underrepresented minority populations [5, 8]. In fact,
the US National Cancer Institute did not begin
collecting socioeconomic information on cervical cancer
patients until the mid-1970s [9].
In 1974 and 1975 Dr. Stern designed a series of survey
studies with colleagues in the UCLA School of Public
Health. [10, 11]. The stated goal of this research was
to determine how Pap testing frequency was related to
cervical cancer rates and socioeconomic factors,
particularly race, ethnicity, and income. This
information could be used to determine the effectiveness
of Pap testing as a screening tool and how often it was
used by different communities.
Prior to conducting these surveys, Dr. Stern and her
colleagues integrated existing data from different
sources to generate a comprehensive view of how cervical
cancer differentially affected Los Angeles
neighborhoods. This included publicly available records
on cervical cancer frequency and associated deaths and
US Census data about income, race, and ethnic
distribution. Their research found that the rates of
cervical cancer diagnosis and mortality were twice as
high as among lower-income, inner city Los Angeles
neighborhoods compared to middle income areas.
The subsequent surveys focused on three representative
communities:
• A low-cancer rate, middle-income neighborhood with
equal representation among white, Latina, and Black
women; 321 women were interviewed.
• A high-cancer rate, low-income neighborhood; 33% of
respondents were Latina and 64% were white; 179 women
were interviewed.
• A high-cancer rate, low-income, inner-city
neighborhood; 98% of respondents were Black; 200 women
were interviewed. The surveys found that, along with elevated cervical
cancer rates, women from lower income areas reported
having fewer Pap tests. Only one-third of low-income
women had been tested twice in the past five years
compared to about 90% of middle-income women. These
differences seemed to be more dependent on income as
opposed to race and/or ethnicity, as all women from the
middle-income groups had increased rates of Pap testing.
However, within poorer communities, Latinas had the
lowest rates of Pap testing with 24% never having had a
Pap test as contrasted with 5% to 12% of Black and white
women. Overall, these surveys reflected serious
disparities in women’s healthcare that needed to be
addressed.
Developing Guidelines for Engaging At-Risk Communities
in No-Cost Cancer Screening Clinics
The ultimate goal of the surveys was to identify key
areas for establishing a community-based cervical cancer
screening clinic [12] with the aims of:
• Determining if women were interested in free cancer
screening.
• Identifying strategies that would help engage women to
make and keep appointments.
• Demonstrating how clinics can function as part of the
community.
• Establishing methods for training healthcare workers
to effectively communicate with patients.
As part of this study, Dr. Stern and her colleagues
asked Los Angeles County public health professionals for
advice in approaching potential patients and advertising
no-cost clinic services. Based on this feedback, Dr.
Stern’s group offered additional services such as breast
exams along with Pap testing. These healthcare
professionals were women from the local communities who
were able to understand patient concerns and explain
medical procedures and results in a relatable manner.
Many could also speak Spanish, which was essential,
since one of the clinic sites was in a Spanish-speaking
neighborhood.
Recruiters went door-to-door, visiting more than 1,200
households in the two low-income areas from the survey
studies described above. Of the 500 women that were
eligible, one third made and kept appointments, a high
success rate for a two-week pilot study. To help women
keep appointments, Dr. Stern’s group provided a wide
variety of free services including taxi rides and
on-site babysitting as well as evening appointments. The
taxi service was used by a third of participants,
highlighting the crucial role of transportation in
healthcare access.
They also hired a woman nurse practitioner to perform
the Pap tests and pelvic exams, which was unheard of at
the time. The patients appreciated this effort and in
post-visit questionnaires, 77% of the women said they
would prefer a female nurse or doctor to perform a
similar exam in the future.
Fifty percent of the women they screened had not had a
Pap test in the previous two years, and 30% of the
Latina women had never had a Pap test. The fact that Dr.
Stern and her group made these efforts in the 1970s
speaks to their progressive mindset and dedication to
helping patients.
Long-Term Impact and Conclusions
Dr. Stern’s forward-looking focus on communication and
empathy was evident in an article which quotes a
healthcare worker from the clinic [12]:
“A worker must know what she is talking about. She
should be friendly and easy going and should not be like
an officer taking down information. The women live in an
area where crime is high and you have to let them know
you are in their neighborhood for a purpose. You have to
know when women don’t want to talk…When you can laugh
with a woman and she sees that you like her and her
children, then she’ll begin to trust you. Once you start
to communicate, she’ll accept an appointment.”
This quotation in one of Dr. Stern’s last published
papers reflects the importance of working within a
community to advance public healthcare policy.
Footnotes:
These numbers are derived from the NIH National Cancer
Institute’s
SEER database (Surveillance,
Epidemiology, and End Results Program). This site
provides long-term and short-term trends for specific
types of cancer including statistics relating to
frequency, survival and mortality. These data can be
filtered by patient sex, age, race, ethnicity or stage
of cancer at diagnosis. SEER began collecting cervical
cancer mortality data in 1975 but the major drop in
deaths from Pap testing in the 1960s and early 1970s
isn’t fully captured by this data.
The average 5-year survival rate for cervical cancer
across all stages of cervical cancer diagnosis and all
patients is at 66.3%. However, for the earliest stage of
cervical cancer (termed “localized” on the SEER
website), the 5-year survival rate is greater than 90%.
These statistics are frequently updated and the numbers
reported here reflect 2011-2017 trends.
In addition to questions relating to differences in
cervical cancer rates and mortality across different
income, racial, and ethnic groups, there was a broader
issue in the field. Many physicians didn’t believe the
Pap test was the reason cervical cancer death rates were
plummeting [7]. There were no coordinated clinical trial
efforts. Such double-blind studies would have been
challenging, making it difficult to determine the
precise impact of the Pap Test [1]. Skeptics of
cytopathology were dubious of these claims [13], as well
as the link between dysplasia and cervical cancer.
However, today the Pap test is widely regarded as a
vital tool in reducing cervical cancer incidence and
deaths.
Dr. Stern’s former graduate students,
Dr. Marilyn Winkleby (Professor of
Medicine, Stanford Prevention Center) and
Dr. Anna Wu (Professor of
Preventive Medicine, Keck School of Medicine at USC)
were consulted to place her research in context.
Other articles published at this time often focused on
the attitudes of women who did not show up for
screenings, often casting them in a negative light. For
example, a 1970 report on cervical cancer screenings in
Louisville, Kentucky [6] stated: “It is quite obvious
that this older group of women present a problem. They
seem recalcitrant to screening, usually have advanced
disease, and, consequently, contribute appreciably to
the difficulty in obtaining a dramatic drop in death
rate.”
See Footnote #2. Dr. Stern was also interested in
using this data to help improve the efficacy of the Pap
test in reducing mortality from cervical cancer, adding
to the growing evidence that the Pap test was a
successful public health tool.
Due to the issues with Pap testing standardization at
the time, including technical problems and physician
errors, annual testing was crucial for continuous
monitoring.
This is still true today. See
this review [14].
References:
1.
Safaeian, M., D. Solomon, and P.E. Castle,
Cervical cancer prevention--cervical screening: science
in evolution. Obstet Gynecol Clin North Am, 2007. 34(4):
p. 739-60, ix.
2.
Kegeles, S.S., et al., Survey of beliefs about
cancer detection and taking Papanicolaou tests. Public
Health Rep, 1965. 80(9): p. 815-23.
3.
Lundin, F.E., Jr., et al., Morbidity from
cervical cancer: effects of cervical cytology and
socioeconomic status. J Natl Cancer Inst, 1965. 35(6):
p. 1015-25.
4.
Breslow, L. and J.R. Hochstim, Sociocultural
Aspects of Cervical Cytology in Alameda County, Calif.
Public Health Rep, 1964. 79: p. 107-12.
5.
Martin, P.L., Detection of Cervical Cancer; a
Study of Motivation for Cytological Screening. Calif
Med, 1964. 101: p. 427-9.
6.
Christopherson, W.M., et al., Cervix cancer
control in Louisville, Kentucky. Cancer, 1970. 26(1): p.
29-38.
7.
Cramer, D.W., The role of cervical cytology in
the declining morbidity and mortality of cervical
cancer. Cancer, 1974. 34(6): p. 2018-27.
8.
Burns, E.L., et al., Detection of uterine
cancer. Results of a community program of 17 years.
Cancer, 1968. 22(6): p. 1108-19.
9.
Singh, G.K., et al., Persistent area
socioeconomic disparities in U.S. incidence of cervical
cancer, mortality, stage, and survival, 1975-2000.
Cancer, 2004. 101(5): p. 1051-7.
10.
Stern, E., et al., Papanicolaou testing and
hysterectomy prevalence in low-income communities: a
survey in Los Angeles County. Natl Cancer Inst Monogr,
1977. 47: p. 113-9.
11.
Stern, E., et al., "Pap" testing and
hysterectomy prevalence: a survey of communities with
high and low cervical cancer rates. Am J Epidemiol,
1977. 106(4): p. 296-305.
12.
Misczynski, M. and E. Stern, Detection of
cervical and breast cancer: a community-based pilot
study. Med Care, 1979. 17(3): p. 304-13.
13.
Guzick, D.S., Efficacy of screening for cervical
cancer: a review. Am J Public Health, 1978. 68(2): p.
125-34.
14.
Scarinci, I.C., et al., Cervical cancer
prevention: new tools and old barriers. Cancer, 2010.
116(11): p. 2531-42. |
|
|
|
|
|
|