 |
 |
 |

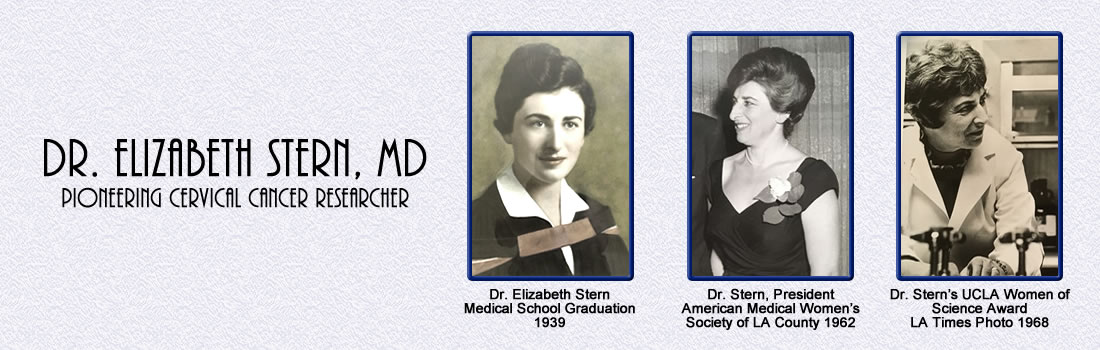
Dr. Elizabeth
Stern
Medical School Graduation 1939 |
In a recent issue of
Scientific American, Dr. Elizabeth Stern was identified
as “probably one of the most significant
physician-scientists who worked at the interface of
epidemiology and cancer in the mid-20th century … her
groundbreaking research led the way to our modern
understanding of the prevention, diagnosis and treatment
of cervical cancer.”
1
Dr. Elizabeth Stern (1915-1980) was an important
contributor to the fields of cytopathology and
epidemiology, two emerging fields of research toward the
mid- twentieth century.
• Cytopathology refers to the diagnosis or detection of
disease at the cellular level, such as through the use
of tissue biopsies or analyzing individual cells. These
studies can be used to determine the stage of disease,
assign appropriate treatment, and monitor patient
progress over time. •
Epidemiology is the study of disease distribution
within and across populations to discover patterns
related to socioeconomic status, age, sex, geographic
location, and other factors. The results of
epidemiological research help guide public health
policy. Dr. Stern was a careful, thorough and meticulous
observer applying techniques from both cytopathology and
epidemiology, publishing over 45 papers. She developed
cytological criteria that enabled detection of
early-stage cervical cancer, allowing earlier treatments
and reducing patient deaths.
Dr. Stern’s research defined the earliest stage of
cervical cancer development, known as cervical
dysplasia, and demonstrated the systematic progression
of cells from this stage to invasive cancer [1].
Although not widely recognized at the time, dysplasia is
now a conventional pre-cervical cancer indicator, and
patients with cervical dysplasia are closely monitored
for signs of progression to cancer.
Dr. Stern’s work on cervical cancer and dysplasia is
tied to her studies on birth control pills. Original
forms of birth control pills contained 10 to 100 times
more estrogen than safe, leading to harmful side effects
largely neglected by the medical profession at that
time. Dr. Stern found that high-dose birth control pills
were linked to increased risk of dysplasia and cervical
cancer [2]. This finding coincided with the growing
consumer advocacy movement regarding birth control pills
and together these led to reformulation of pills with
lower and safer estrogen levels.
In terms of cancer epidemiology, Dr. Stern was well
aware that rates of cervical cancer were substantially
higher in poor as opposed to middle- and upper-income
neighborhoods. She worked closely with public health
researchers to establish guidelines for successful
community cervical cancer screening clinics in
underserved areas. Many of her suggestions such as
offering childcare and/or transportation remain relevant
today. Her focus on empathy and clear communication were
years ahead of her time [3-5].
Dr. Stern also worked on improving the Pap test . Her
research with the Jet Propulsion Laboratory streamlined
the processing of cervical tissue samples, leading to
faster and more accurate diagnoses using digital,
automated analysis of Pap tests [6-8]. Dr. Stern’s
contributions were essential to the current version of
the Pap test used today in hospitals, clinics and
cytopathology labs around the world, and have had a
major role in reducing cervical cancer rates in the
United States and abroad.
Early Life and Education
Elizabeth Stern was born in Cobalt, Ontario, Canada, the
fifth of eight children, to parents George and Sarah
Stern. George Stern (1883-1948) was from the Pale of
Settlement in western Imperial Russia, an area
officially designated for Jews and beyond which Jewish
residency, permanent or temporary, was generally
prohibited. Sarah Morgenstern (1883-1964) was from Lodz,
located in the same region. The two married in the early
1900s and their first two children were born in Lodz.
George immigrated to Canada in 1905 to avoid
conscription into the Russian army, which at the time
mandated Jewish men serve 25 years. After immigrating,
George found work in Cobalt, a rapidly growing mining
town in northern Ontario. His first job was paymaster in
a silver mine employing mostly Slavic workers, and this
job may have been related to his fluency in both Slavic
languages and English. George later became the owner of
a grocery store in Cobalt.
Sarah and their first two children joined George in
Cobalt in 1911 where Elizabeth was born in 1915. In
1916, the family made a final move to Toronto, where the
rest of their children were born. George owned a candy
factory for many years while Sarah was deeply involved
in charity work throughout her life in Toronto.
Sarah and George had four sons and four daughters.
Remarkably, all four of their daughters went to
university in Canada and achieved advanced degrees (MD,
DDS, MA), despite restrictive admittance quotas for
women and Jews. None of the four boys went to
university, largely due to economic circumstances during
the Depression.
Elizabeth graduated from high school at age 15 and
attended the University of Toronto for her undergraduate
and graduate degrees. She earned her M.D. in 1939 at age
23, one of only 11 women, and the only Jewish woman in
her graduating class of 125.
While earning her medical degree, she met Solomon
Shankman, who was also attending the University of
Toronto. He earned a Ph.D. in chemistry in 1939.
Elizabeth and Sol married in 1940, eventually settling
in Los Angeles, California, where they had three
children: Paul (1943), Janet (1946), and Anne
(1950-1993).


Dr. Stern, 3rd row from bottom, 4th
image from right |
Professional Life and Contributions
Following medical school, Dr. Stern entered a graduate
studies program at the University of Pennsylvania School
of Medicine from 1941 to 42 focusing on gynecology and
obstetrics. She then moved to Los Angeles where she
entered her residency in pathology in 1942 at Cedars of
Lebanon and Good Samaritan Hospitals, graduated in 1946
and was subsequently certified by the American Board of
Pathology.
After her residency, Dr. Stern continued as an associate
pathologist at the Cedars of Lebanon Hospital from 1946
to 1949. In 1950 she became Director of Laboratories and
Research at the Cancer Detection Clinic of the Cancer
Prevention Society in Los Angeles and held this position
until 1960. It was at this center that Dr. Stern began
her groundbreaking research that occurred during an
important transition point in the study of cervical
cancer.
In 1950, the Pap test was not yet widely implemented
even though cervical cancer was the
leading cause of cancer-related death
among American women [9]. Like many clinics, the Cancer
Detection Center began offering Pap tests in the early
1950s, with increasing numbers of women deciding to have
the test throughout the 1950s and 1960s. Dr. Stern
witnessed firsthand how the Pap test could be used to
diagnose cancer at earlier, more treatable stages, and
recognized its potential to reduce patient mortality
[10].
She was interested in carefully defining the multiple
stages of cervical cancer as there was not a commonly
accepted standardized reference for how to interpret Pap
test results in the mid-twentieth century. This work was
essential for advancing this emerging field of medical
science and for women’s health.
The Cancer Detection Center screened thousands of women
in Los Angeles each year. Her first peer-reviewed
article, “Cytologic Detection of Uterine Cancer in a
Cancer Detection Clinic” (1954) included Pap testing
results from more than 12,000 women from 1952 to 1953
[10].
In 1961, Dr. Stern was the Research Coordinator for the
Project on Hormone Metabolites in Cancer at the
University of Southern California Medical School and was
hired as the Chief of Cytology in the Department of
Pathology at the UCLA Center for Health Sciences. The
first year of her work at UCLA was unpaid. Although she
had been offered a paid position at another institution,
she ultimately declined the offer, as it would have
taken her away from her family for much of each year.
In 1963, she moved to the recently established School of
Public Health at UCLA as an associate researcher in a
non-tenure-track faculty position. This meant that she
was required to fund her own research. Dr. Stern’s
transfer to the School of Public Health and her
non-tenure track position reflected the slow recognition
of cytopathology in medicine.
Her lab continued analyzing thousands of patient samples
from local clinics in Los Angeles, resulting in many
peer-reviewed papers [1, 2, 11-13]. One of the major
results of this work was her 1974 paper, “A Cytological
Scale for Cervical Carcinogenesis”, that provided
detailed descriptions for defining cervical cancer
stages from Pap tests and cervical biopsies [1]. Her
multi-year studies also demonstrated the link between
abnormalities in cervical cell shape and size and risk
for cervical cancer. Although controversial at the time,
the association of dysplasia to cervical cancer is now
generally accepted throughout the scientific community.
In 1965, Dr. Stern was promoted to Associate Professor
in Residence, and in 1972 was made Professor in
Residence at the UCLA School of Public Health. At this
point, she was collaborating with numerous researchers
in epidemiology, biostatistics, pathology, and public
health, expanding her studies of cervical cancer and
receiving professional recognition including: President
of the American Medical Women’s Association of Los
Angeles County, Branch 23 (1962), Fellow of the College
of American Pathologists (1963), UCLA Woman of Science
(1968), and International Academy of Cytology Fellow
(1971). She was a founding member of the American
Society of Preventative Oncology.
In 1977, Dr. Stern published the results of a seven-year
study that found a six-fold increase in cervical cancer
for women on the high-dose estrogen birth control pill
[2]. This disturbing discovery combined with growing
evidence of other dangerous side effects, like blood
clots, supported the reformulation of a safer,
lower-dose pill [14].
In the latter part of her career, Dr. Stern broadened
her research to encompass other problems impacting
cervical cancer. Although cervical cancer rates had
dropped substantially in the US by the 1970s, this drop
was not uniform across all communities. Dr. Stern and
her colleagues found that in Los Angeles, the highest
rates of cervical cancer and the lowest rates of Pap
testing occurred in low-income neighborhoods.
The best way to address these issues was through public
policy in order to educate patients on the importance of
cancer screening and to make these tests available to
underserved communities. Dr. Stern helped pilot a
community-based clinic to determine the strategies that
would make these efforts successful in the long term. In
addition to offering free cervical and breast cancer
screening, she noted the importance of follow-up calls,
free transportation, childcare, and flexible scheduling
[3-5]. Her report also stressed the need for bilingual
nurses or doctors who could more personally communicate
with patients, contributing to a more empathetic style
of patient care.
Dr. Stern was also interested in improving the speed and
accuracy of Pap testing, as the process of cell
collection, staining, and analysis had changed little
since the test was developed. She worked with the Jet
Propulsion Laboratory, under the management of the
California Institute of Technology, to develop a system
for digital, automated analysis of Pap tests. As part of
this work, she established an innovative, liquid-based
sampling technique for Pap testing, which removed
non-cervical cells and other debris, making the Pap test
easier to analyze [6-8]. This technique represents one
Dr. Stern’s most lasting legacies, as it paved the way
for an entirely new version of the Pap test, the Liquid
Based Pap test, which continues to be used in hospitals,
laboratories, and clinics around the world today.
Later Life
Dr. Stern worked at UCLA for 20 years and was known as a
brilliant scientist, as well as an excellent mentor and
role model. Colleagues thought that she was ahead of her
time in terms of her pioneering research on cervical
cancer, her concern for the health and well-being of
low-income, underserved communities, and her support of
women scientists. Yet like so many women scientists,
her contributions have been widely under-recognized.
In 1980 Dr. Stern passed away at home from stomach
cancer. As a dedicated scientist, she worked on
manuscripts and corresponded with colleagues up to the
week before her passing. Following her death, Dr.
Dorothy Rosenthal continued their research on improving
the Pap Test, working with the Jet Propulsion Laboratory
to complete these studies. Unfortunately, Dr. Stern’s
other projects remained unfinished, and her scientific
biorepository, including carefully curated slides
denoting unique stages of cervical cancer, has been
lost.
Just prior to her death, the UCLA School of Public
Health Division of Epidemiology established and endowed
The Elizabeth Stern Cancer Epidemiology Lectureship to
be awarded annually. Dr. Stern was able to select the
first speaker. In her memory, Sol Shankman established
the Dr. Elizabeth Stern bursary for women students of
minority status at University of Toronto. In 2014 he
passed away at age 98.
Sources:
Janet Williamson
Ellen Weinzapfel
Paul Shankman
Gail Lord
Laura Lamb
Sandor Stern
Ruth Stern
Janice Kreiger
Kathy Leslie
Ken Castleman
Footnotes:
https://blogs.scientificamerican.com/voices/one-more-pioneering-woman-in-science-youve-probably-never-heard-of/
by Ellen Elliott (Weinzapfel)
Dysplasia refers to mild abnormalities in cervical
cell shape and size. All cervical cancers start with
dysplasia, but dysplasia does not always lead to cancer.
In many cases, the cellular abnormalities resolve on
their own over time. However, it is not possible to tell
which cases of dysplasia will resolve as opposed to
progress to cancer. So, when dysplasia is detected via
Pap test, physicians keep a close eye on the patient to
prevent cancer progression.
Education was heavily subsidized in Canada in the first
half of the 1900s which made it possible for Dr. Stern
and her sisters to attend university. However during
this time most men, including Dr. Stern’s brothers, had
to go into the workforce filling what entry-level jobs,
mostly for unskilled laborers, were available.
The terms “pathology” and “cyotopathology” and
“cytology” are used interchangeably by some experts and
are treated as separate entities by others.
Pathology: The field of medicine
focused on the diagnosis of disease.
Cytopathology, or Cytology for short: A
subset of pathology, focused on the study of cells to
diagnose disease.
Context: The fields of pathology and
cytopathology grew along side each other. This is why
the two terms are often used interchangeably. Further,
most modern subsets of pathology, pulmonary pathology
and renal pathology, are largely based in analysis of
biopsies and/or cells, making them at least partially
cytopathology specialties.
In the text here, the terms “cytopathology” or
“cytology” are used as much as possible to avoid
confusion.
Tenure and non-tenure track positions are very
different in academia. Tenure-track positions are more
desirable and more research-oriented with job security
and higher salaries. Receiving tenure requires a track
record of success in publications, funding, and
teaching. Universities and colleges distinguish these
positions that require a long-term funding horizon and
lifetime employment from non-tenure track appointments
that are typically short-term, pay far less, and focus
on teaching. There are also non-tenure track positions
with a focus on research for faculty members who obtain
external grant funding to support their positions.
As a non-tenured faculty member, she obtained external
funding to supprt her own position in the UCLA School of
Public Health. In addition, she taught courses and was a
graduate student advisor. Despite the lack tenure,
Dr. Stern vigorously pursued and achieved many of her
goals.
From Ellen Weinzapfel’s interviews and correspondence
in 2017 with Dr. Dorothy Rosenthal (Johns Hopkins
University), Dr. Marylin Winkleby (Stanford University),
and Dr. Anna Wu (University of Southern California), all
of whom worked with Dr. Stern at UCLA.
References:
1.
Stern, E., et al., A cytological scale for
cervical carcinogenesis. Cancer Res, 1974. 34(9): p.
2358-61.
2.
Stern, E., et al., Steroid contraceptive use and
cervical dysplasia: increased risk of progression.
Science, 1977. 196(4297): p. 1460-2.
3.
Stern, E., et al., Papanicolaou testing and
hysterectomy prevalence in low-income communities: a
survey in Los Angeles County. Natl Cancer Inst Monogr,
1977. 47: p. 113-9.
4.
Stern, E., et al., "Pap" testing and
hysterectomy prevalence: a survey of communities with
high and low cervical cancer rates. Am J Epidemiol,
1977. 106(4): p. 296-305.
5.
Misczynski, M. and E. Stern, Detection of
cervical and breast cancer: a community-based pilot
study. Med Care, 1979. 17(3): p. 304-13.
6.
Rosenthal, D.L., et al., Endocervical columnar
cell atypia coincident with cervical neoplasia
characterized by digital image analysis. Acta Cytol,
1982. 26(2): p. 115-20.
7.
Rosenthal, D.L., et al., A simple method of
producing a monolayer of cervical cells for digital
image processing. Anal Quant Cytol, 1979. 1(2): p. 84-8.
8.
Stern, E., et al., An expanded cervical cell
classification system validated by automated
measurements. Anal Quant Cytol, 1982. 4(2): p. 110-4.
9.
Safaeian, M., D. Solomon, and P.E. Castle,
Cervical cancer prevention--cervical screening: science
in evolution. Obstet Gynecol Clin North Am, 2007. 34(4):
p. 739-60, ix.
10.
Stern, E. and N.P. Menoher, Cytologic detection
of uterine cancer; in a cancer detection clinic. J Am
Med Womens Assoc, 1954. 9(11): p. 343-9.
11.
Stern, E., Cytohistopathology of cervical
cancer. Cancer Res, 1973. 33(6): p. 1368-78.
12.
Stern, E. and P.M. Neely, Dysplasia of the
Uterine Cervix. Incidence of Regression, Recurrence, and
Cancer. Cancer, 1964. 17: p. 508-12.
13.
Stern, E. and P.M. Neely, Carcinoma and
Dysplasia of the Cervix: A Comparison of Rates for New
and Returning Populations. Acta Cytol, 1963. 7: p.
357-61.
14.
Liao, P.V. and J. Dollin, Half a century of the
oral contraceptive pill: historical review and view to
the future. Can Fam Physician, 2012. 58(12): p. e757-60.
|
|
|
|
|
|
|